Retake
A33) Severe chest pain and dyspnea after MVC
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a trauma patient.
- Review the DDx considerations in trauma patients.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a trauma patient.
History
A 24-year-old male presenting as a trauma alert following a high-speed motor vehicle collision. He reports sudden onset, severe, left sided chest pain and difficulty breathing immediately following the accident. An NG tube was placed en route as the patient was experiencing significant vomiting.
Physical Exam
BP 109/65, HR 118, RR 29, Temp 98.3 F, O2 saturation 92%.
Cardiac: Normal S1, S2. No murmurs, rubs, or gallops. There is no jugular venous distension.
Lung: Decreased lung sounds in the left hemithorax.
Abdomen: Tenderness to palpation over left upper quadrant.
Labs
Unremarkable.
Provisional Diagnosis
Select the Dx you believe is most appropriate
Any of the above diagnoses are possible in this patient with left sided chest pain, respiratory distress, and decreased left sided lung sounds.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient requires urgent workup and management.
First Imaging Study
What is the first imaging study you will order?
A portable chest x-ray performed in the trauma bay would be the best initial imaging modality to evaluate for a pneumothorax, diaphragmatic rupture, or hemothorax. It is quickly obtainable and can rule out life-threatening pathologies in the setting of trauma.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
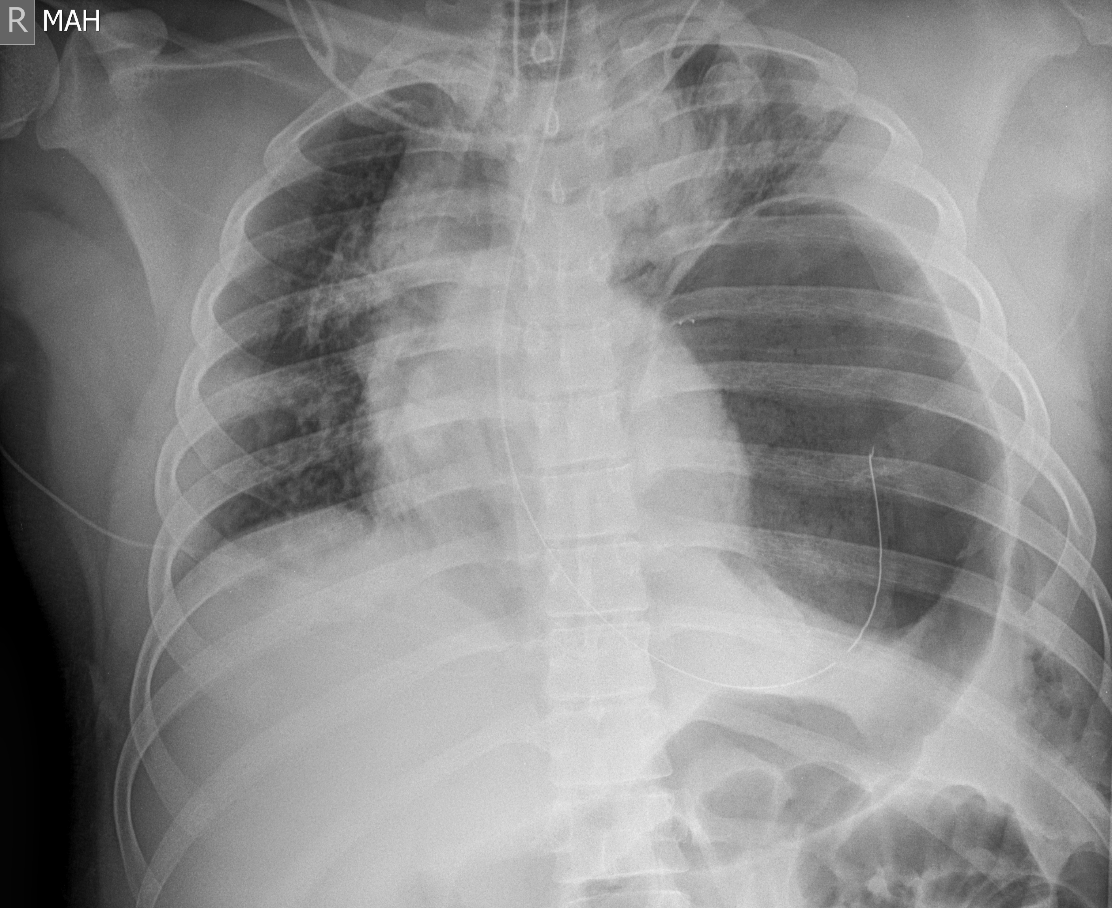
Portable Chest x-ray
Is there a pneumothorax present?
There is no pneumothorax, as there is no visible pleural line, the pulmonary vasculature is present throughout the left chest, and there is no deep sulcus sign.
Is there a hemothorax present?
There is no hemothorax, as there is no blunting of the costophrenic angle to suggest fluid accumulation in the pleural space.
Is there evidence of a diaphragmatic rupture?
There is evidence of a diaphragmatic rupture, as the gastric bubble and the tip of the nasogastric tube, which terminates in the stomach, are located in the left hemithorax.
Is there mediastinal shift present?
There is mediastinal shift, as the diaphragmatic rupture results in rightward deviation of the trachea and mediastinum.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
Diaphragmatic ruptures are often associated with other injuries considering the large amount of force needed for this injury. A CT chest and abdomen would best imaging study to evaluate for these injuries. However, considering that there were no other alarming findings on the primary and secondary examinations, the patient should go directly to the operating room to prevent respiratory compromise and bowel strangulation.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The imaging findings are most consistent with diaphragmatic hernia.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires emergent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
A 24-year-old patient presents following a high-speed motor vehicle accident, with a chest X-ray showing the gastric body and a nasogastric tube in the left hemothorax, indicative of a traumatic diaphragmatic rupture. The patient should emergently undergo exploratory surgery to address the suspected left-sided diaphragmatic rupture and assess for associated injuries. During surgery, the diaphragm should be repaired primarily, or with prosthetic materials if a large defect is present and there is no colonic contamination.
Lessons Learned:
- Symptoms of a diaphragmatic rupture may range from asymptomatic to respiratory distress or signs of bowel obstruction.
- The left diaphragm is more commonly ruptured than the right due to congenital weakness and the liver's protective role on the right side during blunt trauma.
- Chest X-ray findings may include a gastric bubble, bowel loops and/or nasogastric tube in the thoracic cavity, but the X-ray may also appear normal.
- CT scans of the chest and abdomen are more sensitive for detecting diaphragmatic hernias and confirming the diagnosis.
- Delayed diaphragmatic rupture can occur months or even years after blunt trauma, especially in children.
- Surgical repair is necessary for all left-sided diaphragmatic rupture. Some right-sided ruptures may undergo a trial of conservative management.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}